Adductor Canal/Saphenous Block
The saphenous nerve is a terminal branch of the femoral nerve (L3–L4) and is typically blocked within the adductor canal in the medial thigh. It provides sensory analgesia to the medial knee, medial lower leg, and medial ankle while largely preserving motor function. It is often combined with a popliteal/distal sciatic block for complete lower-extremity anesthesia.
Indications: Knee surgery; medial knee pain; lacerations, abscesses, or foreign-body removal of the medial lower leg/ankle; neuropathic pain; ankle fracture or reduction involving the medial malleolus
Considerations & Technical Details
Considerations:
Document a neurovascular exam prior to performing the block.
Do not perform if there is concern for compartment syndrome, especially in the setting of tibial fractures.
Can be performed in tandem with the popliteal / distal sciatic nerve block for complete anesthesia of the lower extremity.
The saphenous nerve is typically considered purely sensory, but the literature suggests possible motor innervation of the vastus medialis. When blocked, this can occasionally result in mild weakness.
Calculate a maximum safe dose of anesthetic prior to the block to avoid LAST.
Transducer: High-frequency linear probe
Needle: 20–22 g, 5–10 cm nerve block needle or short-bevel needle
Anesthetic Volume: 10 mL
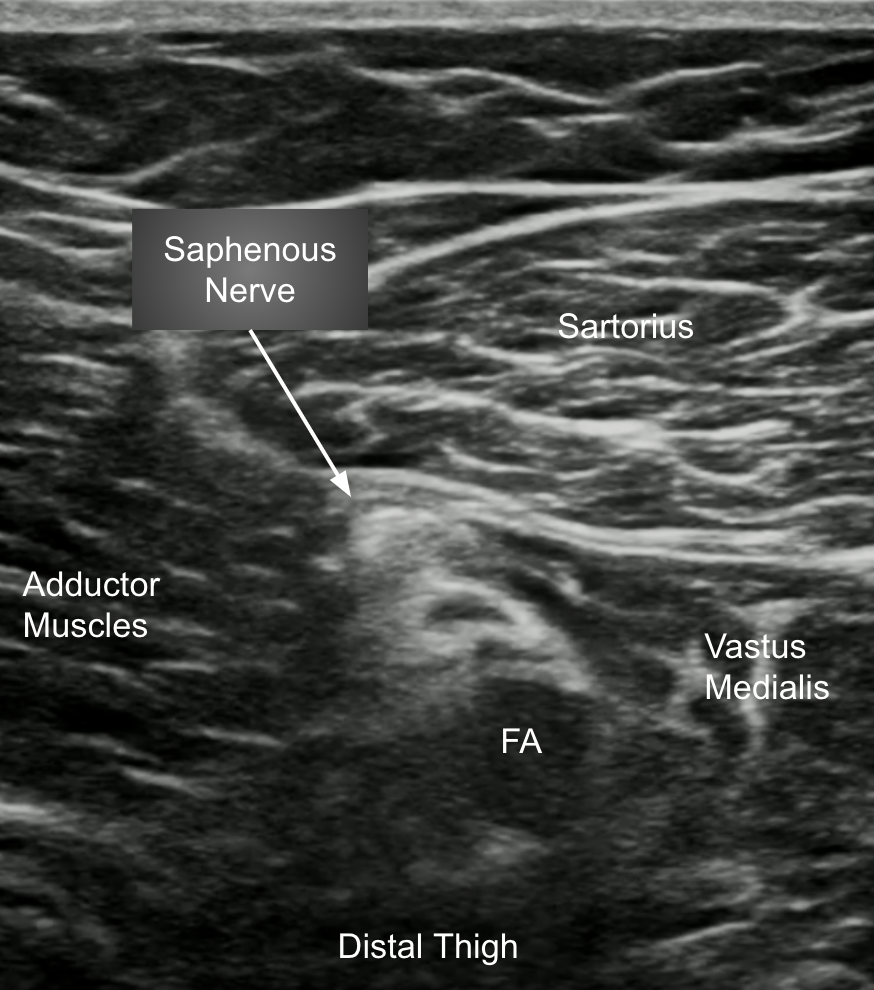
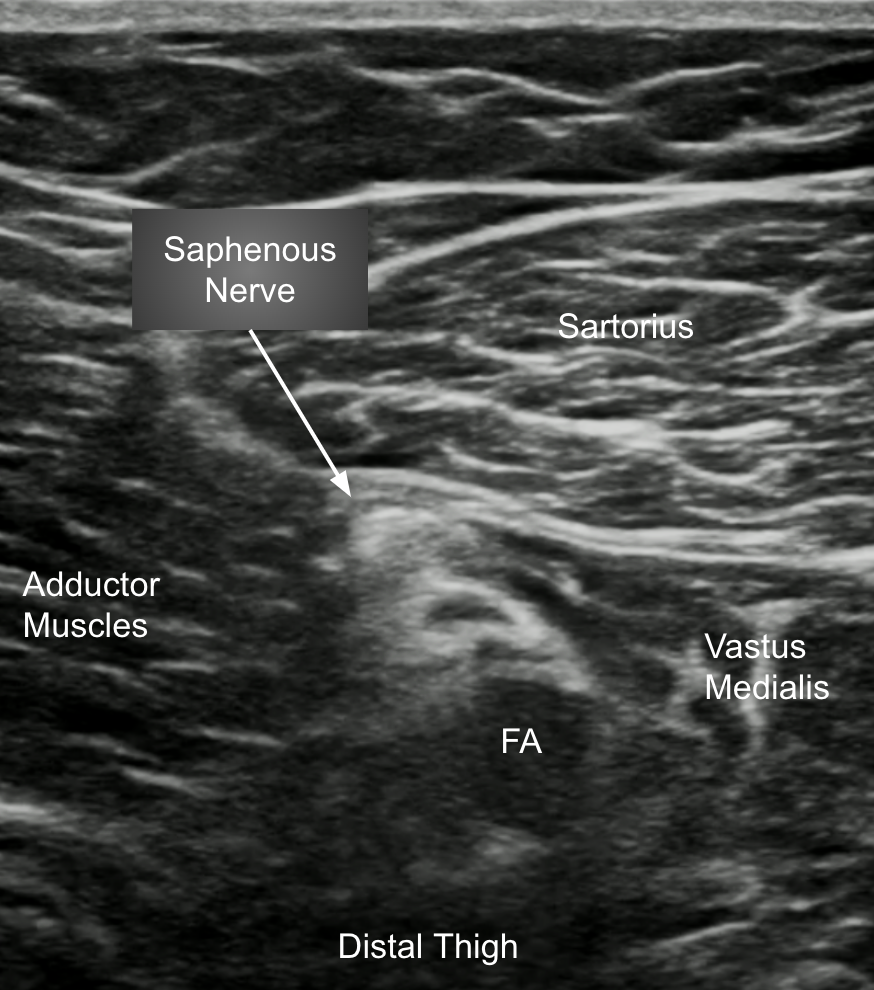
Target of Anesthetic: Anesthetic spread around the saphenous nerve, 5–7 cm proximal to the popliteal crease, deep to the sartorius muscle and anterolateral to the femoral artery
Area of anesthesia
Positioning
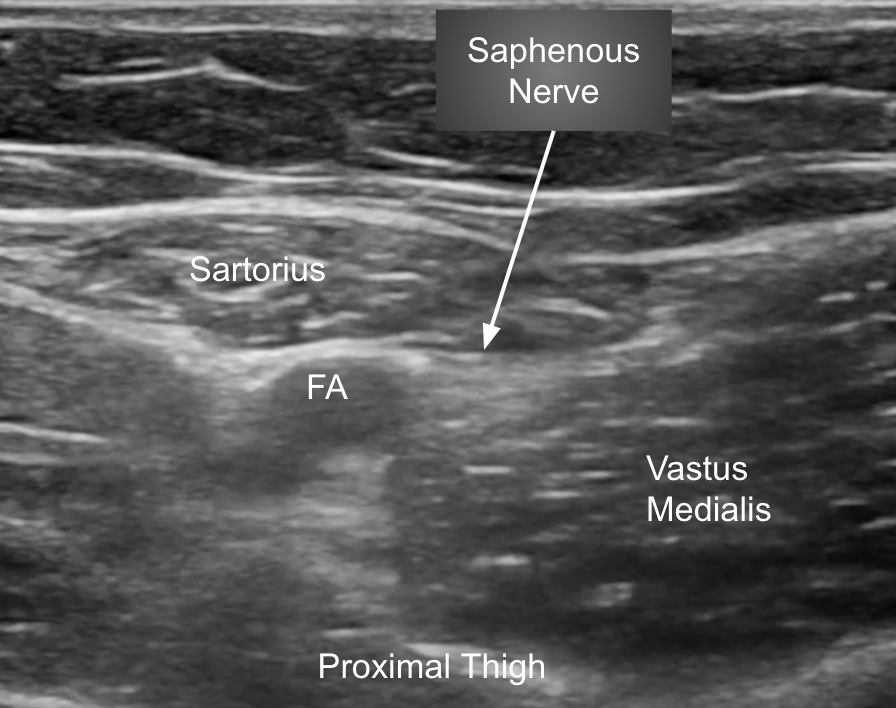
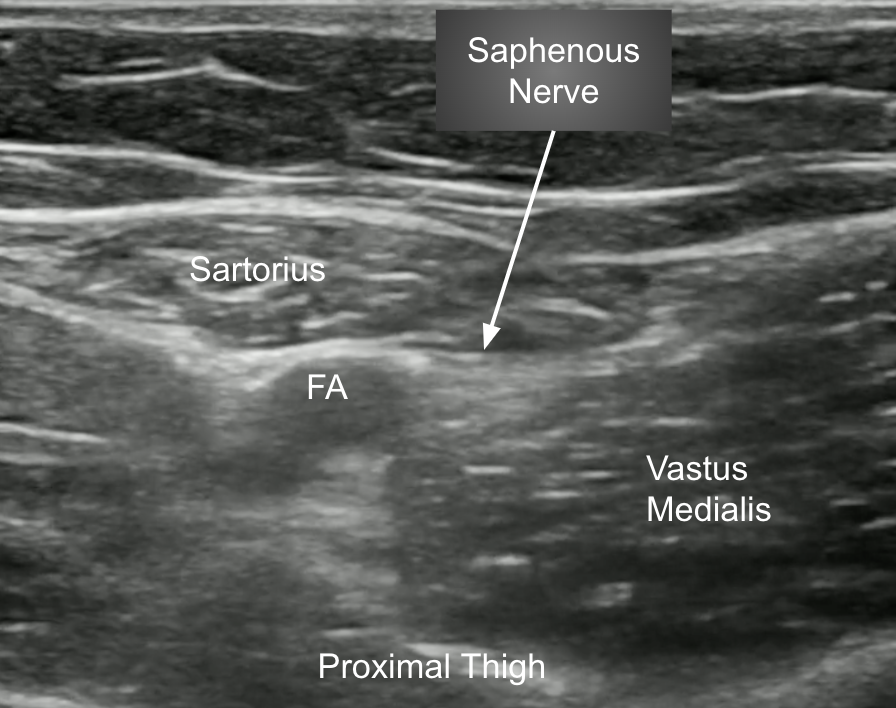
Position the patient supine with the leg abducted and externally rotated. Place the high-frequency linear probe approximately 5–7 cm proximal to the knee on the medial thigh, over the adductor canal, in a transverse orientation.

Target Identification
Identify the sartorius muscle and the femoral artery. The saphenous nerve lies deep to the sartorius muscle and anterolateral to the femoral artery within the adductor canal.
Needle Approach
Advance the needle using an in-plane approach from medial to lateral, into the plane around the saphenous nerve. Deposit ~10 mL of local anesthetic, watching for circumferential spread around the nerve.