Genicular Block
Common Indications: Acute or chronic knee pain
The genicular nerve block targets the small articular branches that supply the anterior compartment of the knee, providing motor-sparing analgesia for acute or chronic knee pain. Because the genicular nerves are small with variable positions, the block relies on bony and vascular landmarks rather than direct nerve visualization. Three injections (superolateral, superomedial, and inferomedial) are required for complete joint coverage.
Considerations & Technical Details
Considerations:
Document a neurovascular exam prior to performing the block.
Motor-sparing.
The genicular nerves are small with variable location and will not be directly visualized. This block uses ultrasound bony and vascular landmarks.
Provides analgesia of the anterior compartment of the knee in each correlating quadrant of the superolateral (SLGN), superomedial (SMGN), and inferomedial (IMGN) nerve distributions — requires 3 injections for complete joint coverage.
There is also an inferolateral genicular nerve that traverses over the proximal fibula, however it is adjacent to the common peroneal nerve. This site is typically not injected due to the risk of common peroneal involvement and resultant foot drop.
Calculate a maximum safe dose of anesthetic prior to the block to avoid LAST.
Transducer: High-frequency linear probe
Needle: 20–22 g, 1.5–3.5 in (3.8–8.9 cm) nerve block needle
Anesthetic Volume: 5 mL per nerve
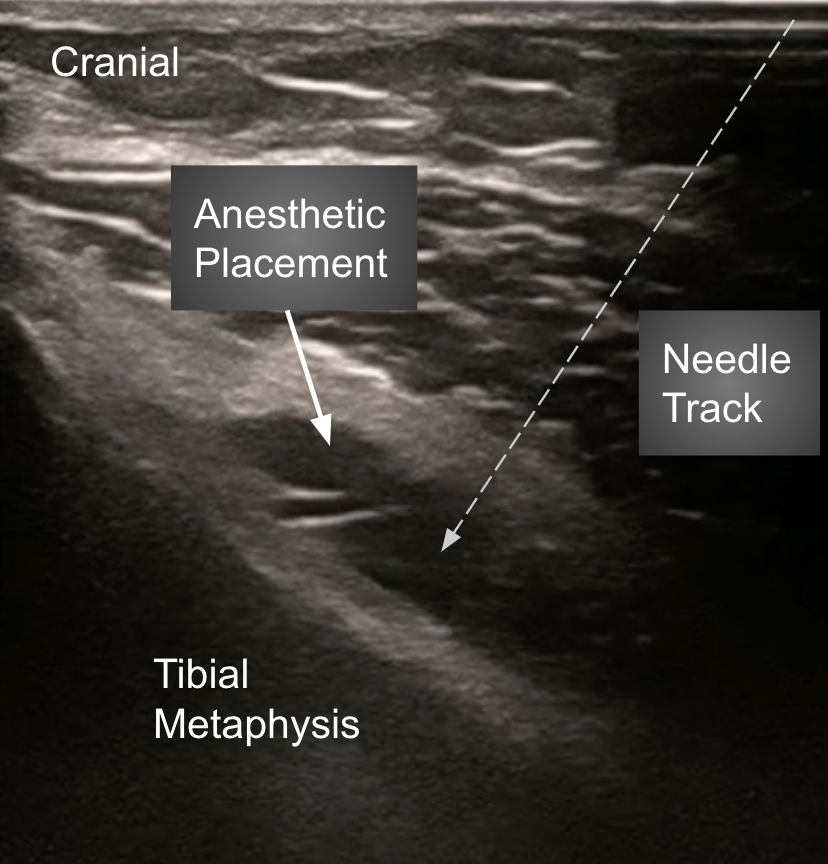
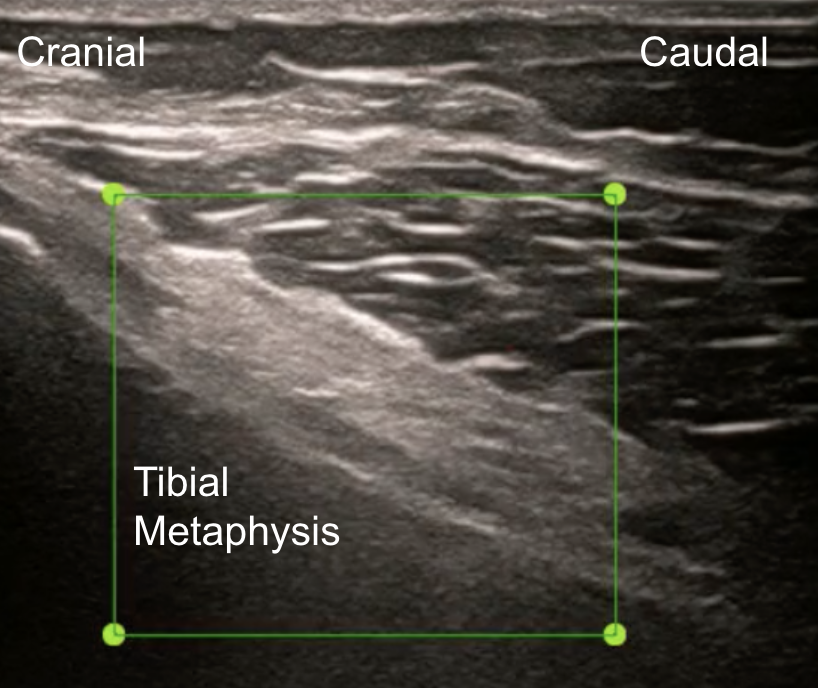
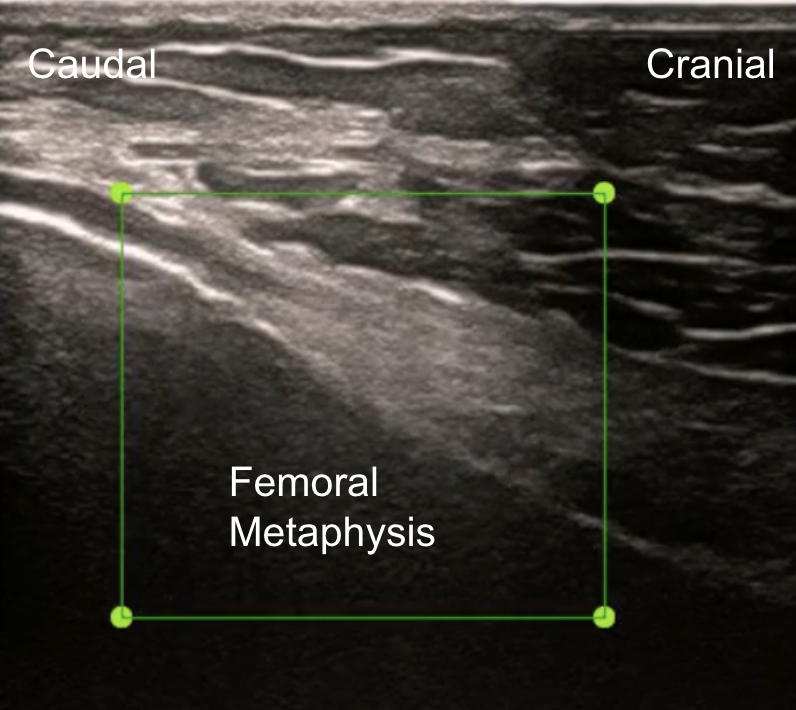
Target of Anesthetic: Anesthetic deposition along the periosteum at the point of upsloping of the long bone (metaphysis–epiphysis junction)
Area of anesthesia
Positioning
Position the patient supine with the knee slightly flexed by placing a pillow in the popliteal fossa. Place the probe with the marker oriented cephalad in a sagittal or slightly oblique plane along the medial and lateral distal femur and the medial proximal tibia.



Target Identification
At each site, identify the long-bone metaphysis — the point of initial osteal upsloping — and look for the adjacent genicular arteries when visible. The three injection targets are the superolateral, superomedial, and inferomedial genicular nerve distributions. Avoid the inferolateral site to prevent common peroneal involvement.
Needle Approach
Use an in-plane technique. For the superior nerves, advance the needle superior-to-inferior; for the inferior nerve, advance inferior-to-superior. Deposit ~5 mL of local anesthetic against the periosteum at each site, lifting the overlying tendons and musculature. Repeat for all three target sites for complete joint coverage.