
Clavipectoral Block
Common Indications: Clavicle Fractures
The clavipectoral fascial plane block deposits local anesthetic between the clavipectoral fascia and periosteum of the clavicle to provide analgesia for clavicle fractures. It is a fantastic block for a very painful clavicle fracture especially in the setting of sports injuries. It offers targeted pain control while avoiding phrenic nerve palsy and upper extremity motor blockade associated with more proximal brachial plexus blocks such as the Superficial Cervical Plexus Block.
Considerations & Technical Details
Indications:
Clavicle fractures
Contraindications:
Infection overlying injection site
Allergy to local anesthetics
Open fracture
Considerations:
Document a neurovascular exam prior to performing the block.
The fascia may be disrupted by the fracture, so this block can be performed on each side of the fracture for more complete analgesia.
Because this is such a superficial block, initial skin entry with a blunt tipped needle may be one of the more challenging parts. Have someone hold the skin taught while you enter the skin, if possible.
Calculate a maximum safe dose of anesthetic prior to the block to avoid LAST
Transducer: High frequency linear probe
Needle: 20-22g 1.5-3.5 in (3.8-3.9 cm) spinal/nerve block needle
Anesthetic Volume: typically 5 mL on either side of fracture (~10cc total)
Area of Anesthesia

Positioning and Landmarks
Patient supine. Linear probe on top of the clavicle with marker to patient head. Probe can be placed anywhere along the clavicle on either side of the fracture. The needle approach is caudal to cranial.
There are two injections on both sides of the fracture!
Target Identification: 2 injections, both sides of the fracture
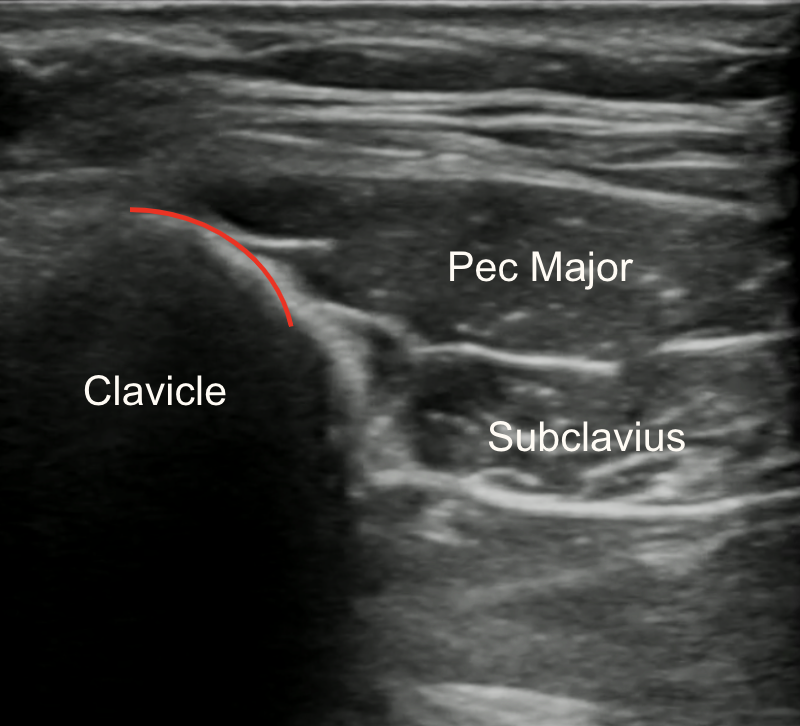
Target of Anesthetic: deposit on top of the clavicle, peeling the fascial layer off of the bone
Identify clavicle and pectoralis muscles
Make note of visualization of ribs and/or pleura
Translate the transducer slightly cephaled to allow space for needle introduction along pectoralis just inferior to the inferior clavicle edge
Needle Approach: Two injections - both sides of the fracture
In-plane needle visualization
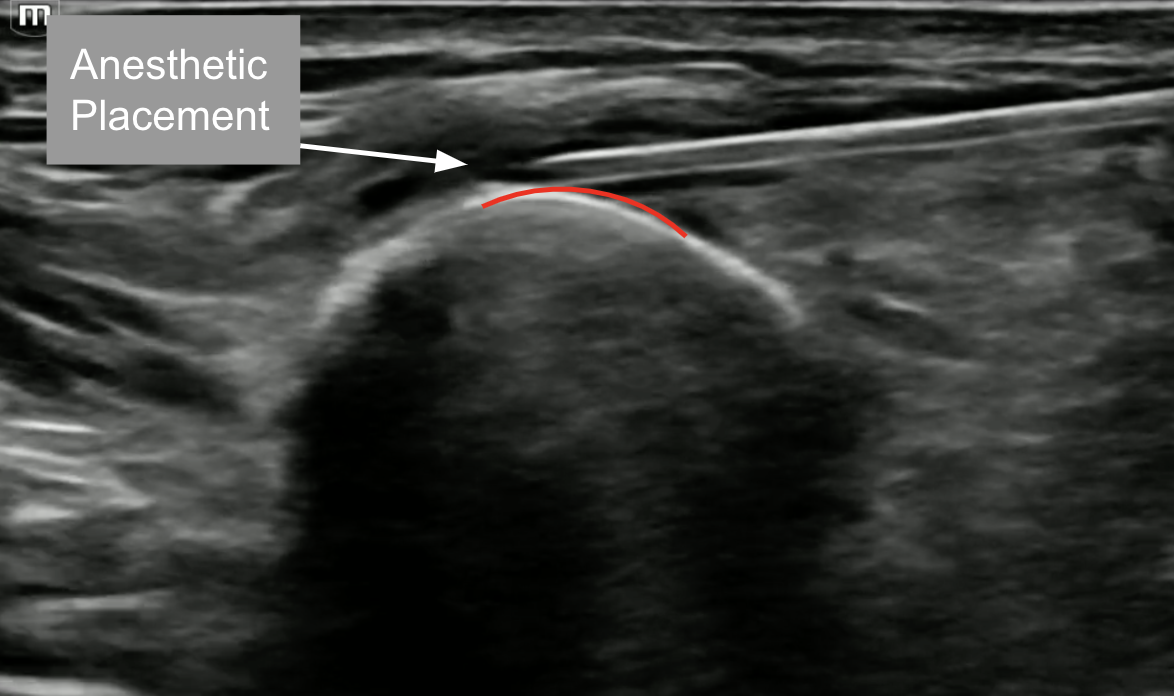
Enter from inferior aspect with the 12 to 2 - o’clock position on the clavicle as your target
Deposit ~ 5 cc of local anesthetic just on top of the clavicle to separate the clavipectoral fascia from the periosteum