
PENG (Pericapsular Nerve Group) Block
The PENG block targets the articular branches of the femoral, obturator, and accessory obturator nerves as they course along the pubic ramus. By depositing anesthetic in the plane deep to the iliopsoas tendon, it provides analgesia for hip and acetabular fractures while preserving quadriceps motor function — a key advantage over the fascia iliaca block for hip-fracture analgesia.
Indications: Fractures of the acetabulum, femoral head, femoral neck, or pelvic rami; hip dislocation
Considerations & Technical Details
Considerations:
Document a neurovascular exam prior to performing the block.
The PENG block will provide analgesia for most hip fractures, fractures of the acetabulum, and pubic rami — an area not covered by the fascia iliaca block.
Coverage is variable for more lateral femoral neck fractures and for intertrochanteric, subtrochanteric, or femoral shaft fractures. In these situations the PENG may not be sufficient and a fascia iliaca block is preferred.
The PENG is motor-sparing, in contrast to the fascia iliaca. However, there are case reports of motor blockade when using more than 20 mL of anesthetic.1,2
Calculate a maximum safe dose of anesthetic prior to the block to avoid LAST.
Transducer: Low-frequency curvilinear probe or high-frequency linear probe
Needle: 18–22 g, 3.5 in (8.9 cm) spinal needle
Anesthetic Volume: 20 mL
Target of Anesthetic: Anesthetic spread along the bony pelvis, lifting the muscle/tendon/fascial layer off the periosteum and under the psoas tendon
Area of anesthesia
Positioning
Position the patient supine and have them externally rotate the affected leg. Place the probe parallel to the inguinal crease at an oblique angle, inferior and medial to the anterior inferior iliac spine.

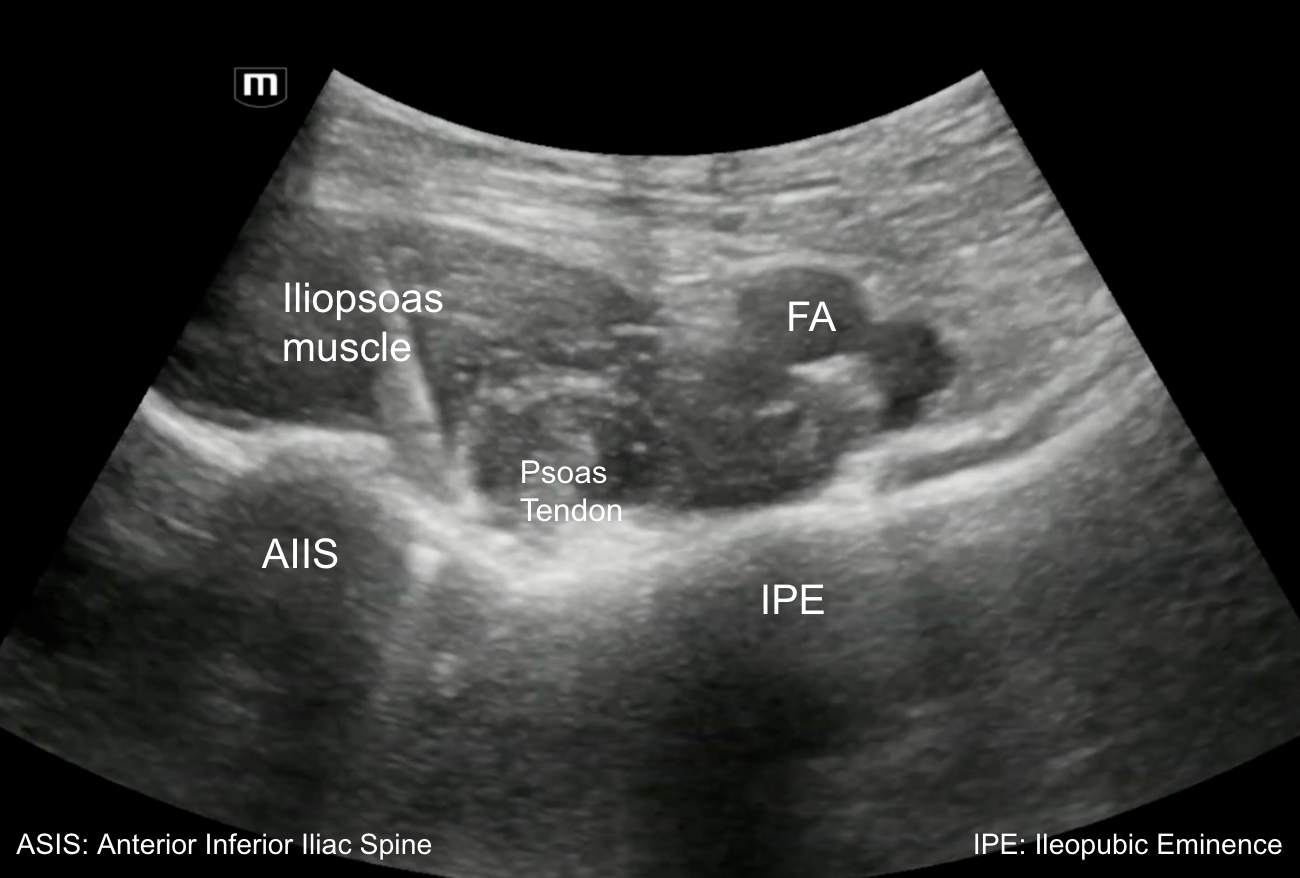
Target Identification
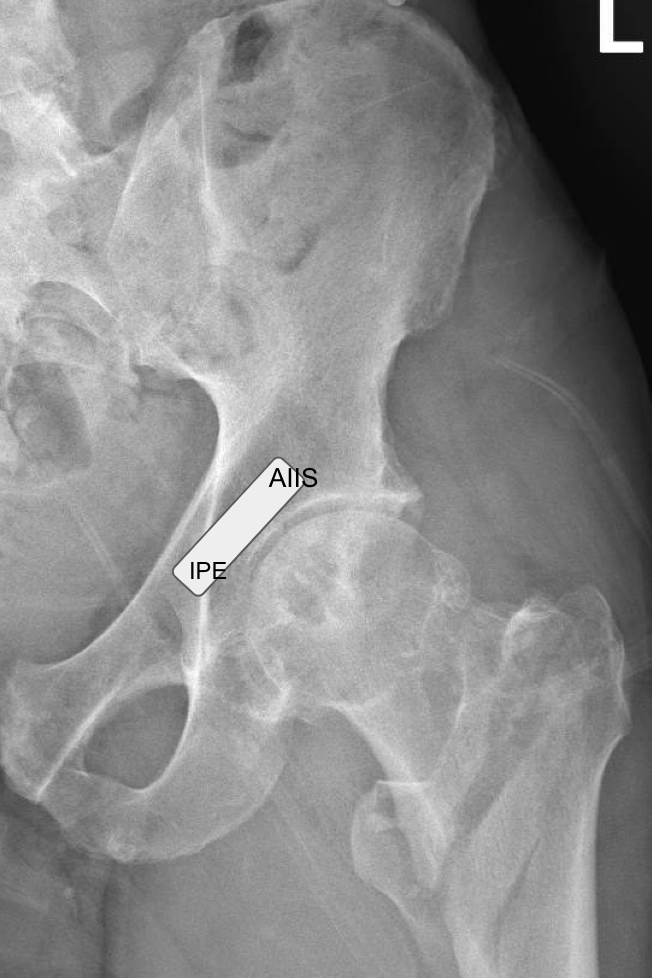
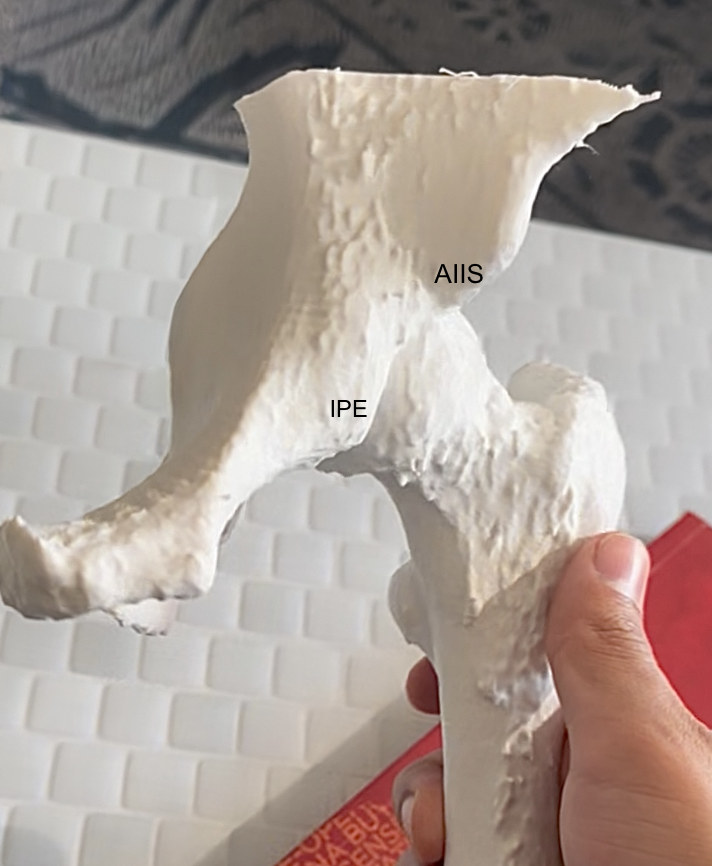
Identify the anterior inferior iliac spine and the iliopubic eminence, with the hyperechoic psoas tendon lying in the bony groove between them. The target plane sits between the psoas tendon and the periosteum of the pubic ramus.
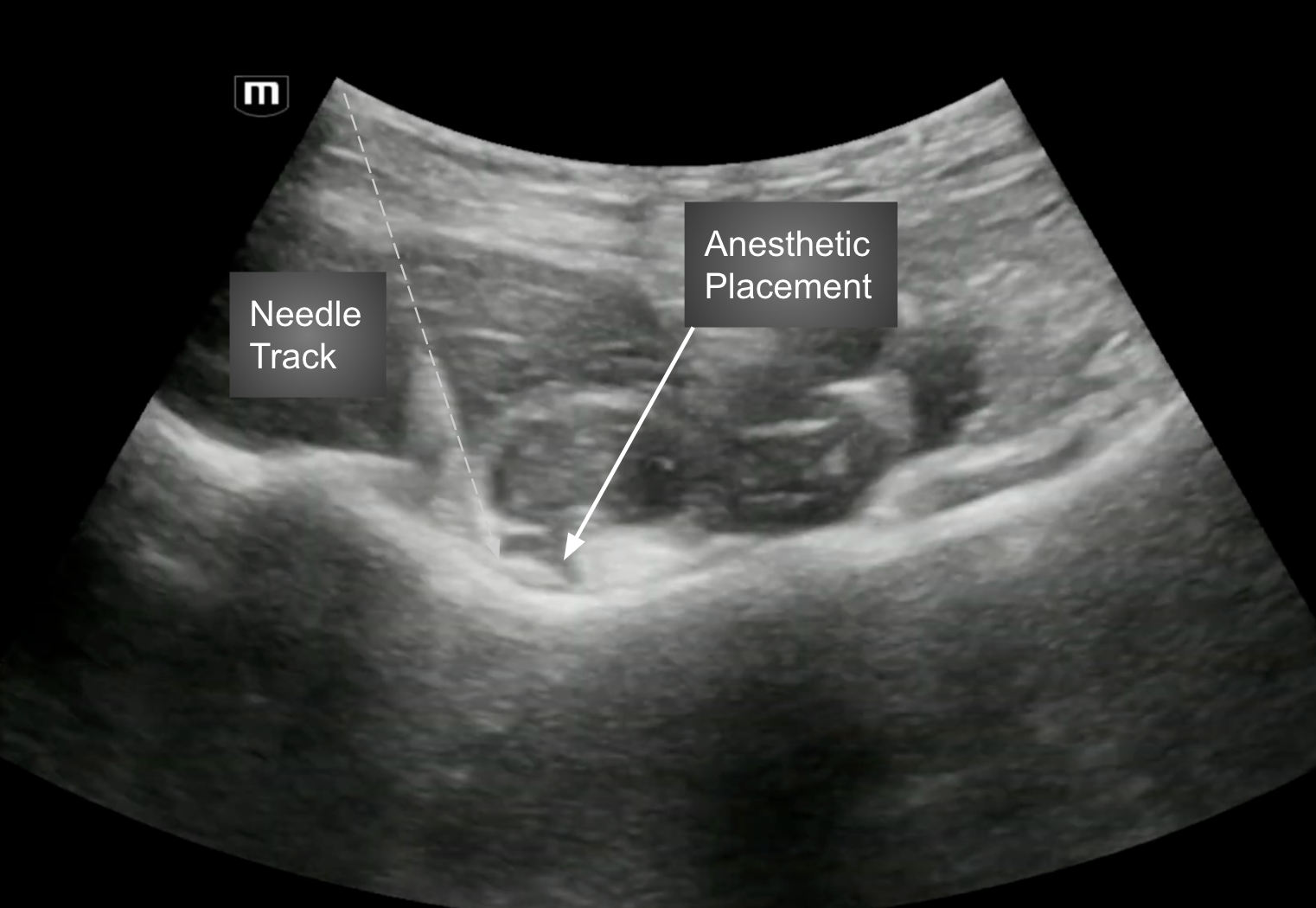
Needle Approach
Using an in-plane technique with a lateral-to-medial trajectory, advance the needle to bone just proximal to and underneath the psoas tendon. Deposit ~20 mL of local anesthetic in this plane to lift the iliopsoas off the bony pelvis.
PENG Videos
Learn More
ACEP Now — Benefits of Using the PENG Block
NYSORA LMS — The Hip: PENG Block
Huang Y, et al. J Pain Res 2024 — Ropivacaine dosing for PENG
Ciftci B, et al. A possible mechanism of motor blockade of high-volume PENG block: a cadaveric study. J Clin Anesth. 2021;74:110407.