Stellate Ganglion Block
The stellate ganglion is a sympathetic ganglion of the cervicothoracic chain that lies at the level of C7–T1, anterior to the longus colli muscle. Ultrasound-guided blockade has been described as an adjunct for refractory ventricular arrhythmia (electrical storm), as well as for chronic-pain indications including complex regional pain syndrome, sympathetically maintained pain, postherpetic neuralgia, phantom limb pain, anxiety, and PTSD.
Indications: Refractory ventricular arrhythmia
Non-emergency-department indications: Complex Regional Pain Syndrome (CRPS), Sympathetically Maintained Pain (SMP), PTSD, anxiety, postherpetic neuralgia, phantom limb pain.
Considerations & Technical Details
Considerations:
The block should be performed on the left side due to a decreased rate of hypotension compared with right-sided blockade.
If there is no improvement after the first block, consider blocking the contralateral stellate ganglion in a similar fashion. A ~10-minute window is reasonable to wait between blocks.
Anchor your hands for stability — CPR will likely be ongoing.
The vertebral artery can run adjacent to or appear to pass through the stellate ganglion. Be alert and use color Doppler before injecting.
Transducer: High-frequency linear probe
Needle: 20–25 g, 5 cm echogenic needle
Anesthetic Volume: 10 mL of a short-acting local anesthetic, such as 1% lidocaine without epinephrine
Target of Anesthetic: Anesthetic spread deep to the prevertebral fascia, between the longus colli muscle and the carotid artery
Positioning
The patient is supine. Turn the patient's head to the right to expose the left side of the neck and to displace the internal jugular vein and other vessels. Anchor your hand during ongoing CPR.


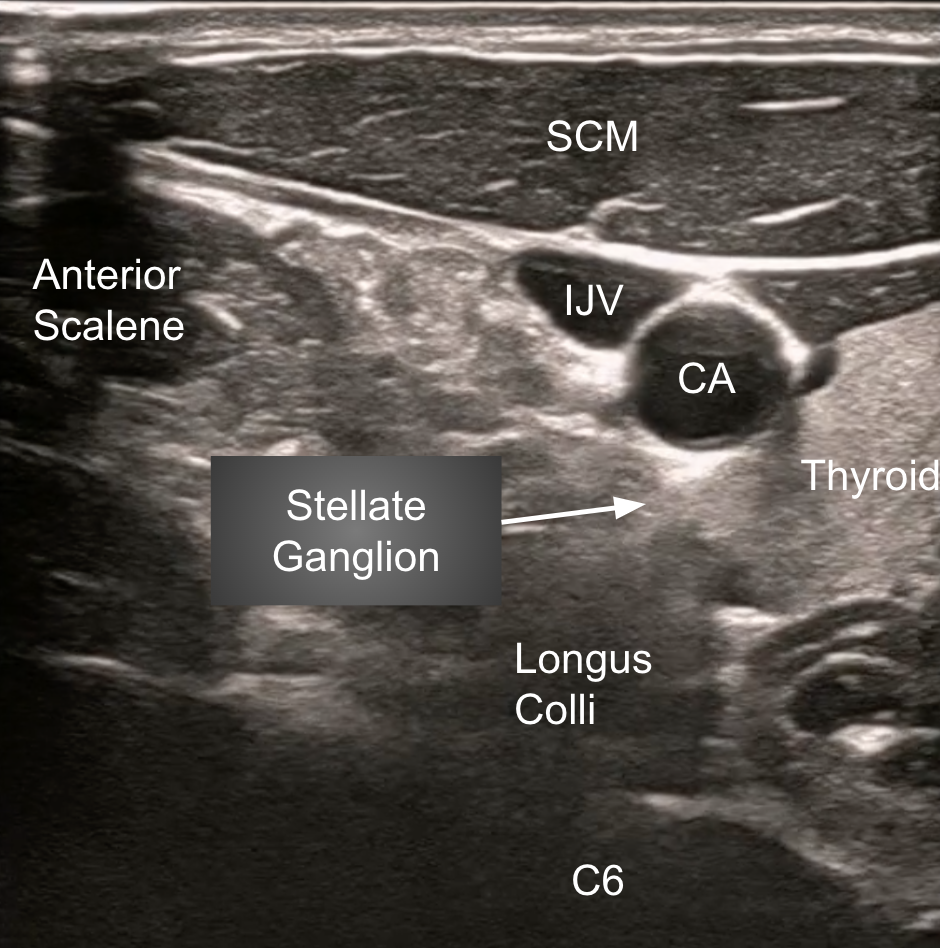
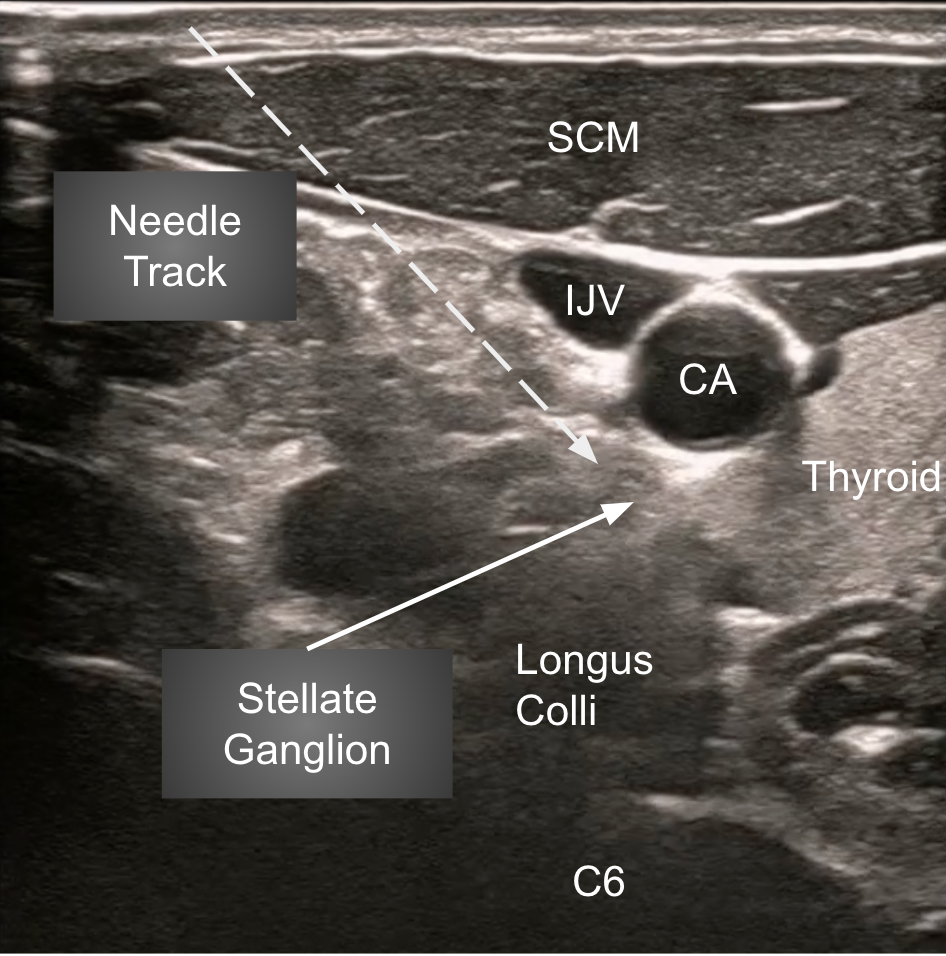
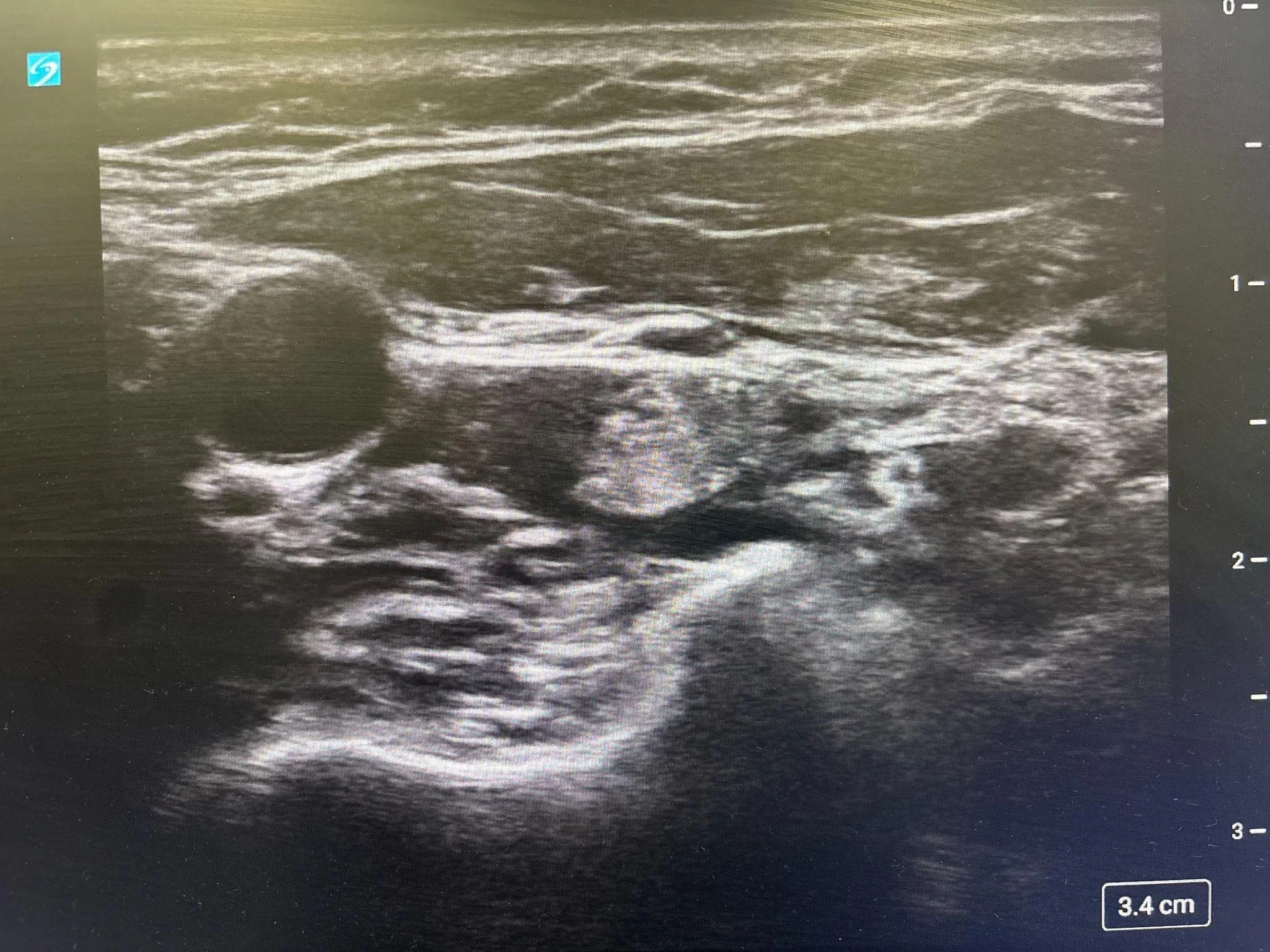
Target Identification
Place the transducer in the transverse plane on the left side of the neck at approximately the C6 level (cricoid cartilage), near where an internal jugular central line would be placed. Identify the carotid artery and, with small cranial-to-caudal sweeps, identify the longus colli muscle deep to it. The injection target sits superficial to the longus colli and just deep to the carotid artery, beneath the prevertebral fascia.
Needle Approach
Consider inserting the needle just under the skin during active compressions, then advancing during a pulse check. Use an in-plane, lateral-to-medial trajectory toward the prevertebral fascia along the superficial aspect of the longus colli, just deep to the carotid artery. Inject 10 mL of short-acting local anesthetic at this target.